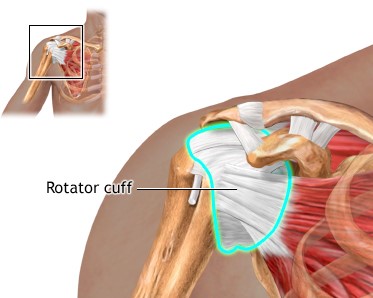
Rotator Cuff
The rotator cuff muscle is a prime muscle in stabilizing the shoulder joint & allows us to lift the arm above the head. Due to wear & tear over time it is common in patients above age of 50 years to develop a rotator cuff tear. Often this tear occurs without any fall or trauma. However, sometimes due to prevailing degeneration within the rotator cuff a trivial trauma – such as fall in bathroom or at times even after a throwing injury. Patients complain of pain at the side of the arm and inability to actively lift the arm.
The rotator cuff tear can be diagnosed either by Ultrasound or MRI examination. If there is a partial tear this can be treated by our PSRP shoulder rehab programme. But once a full thickness tear occurs it can only be treated by surgical repair. Without repairing the tear the shoulder cannot gain function. Local heat or physio does not address the cuff defect. The tear will propagate with time and the later a patient presents the poorer the outcome. Some patients have to be refused surgery as they present too late.
Traditionally rotator cuff used to be repaired with open surgery leading to adhesions and post operative stiffness & recovery generally takes a very long time. At our clinic rotator cuff is repaired arthroscopically with the use of imported suture anchors. After arthroscopic repair, patients go home the next day of surgery & with hardly any scar. Also, working patients tend to join back work within a week of surgery. So far we have hardly have complications with Arthroscopic repair. In our series the chance of re tear especially with patients presenting within few months of tear is less than 1%. Patients presenting late will tend to have a poor quality of muscle to repair.
Typically, patients are admitted the evening before surgery. You may have to book your room well in advance – depending on which hospital you choose to go. Due to hospital rules – they are unable to guarantee a room even though booked.You must come in with an admission letter issued to you when the surgery was decided. Present this at the hospital admission IPD department. The rest of the process is pretty much automatic. One of our Hospital registrars will come in to see you to conform that all the pre-op requirements have been met. He will then mark the arm to be operated with a permanent marker.
If any tests are due then they will be performed. In case you have forgotten any investigation, it is best to draw the attention of the Hospital Doctor who has seen you. Certainly, avoid smoking for a week before surgery and six weeks after surgery. Nicotine has an adverse effect on General anaesthesia. Smoking also retards healing of tissue and re-tear rates are higher in smokers. Avoid alcoholic drinks a day before and after surgery as alcohol counteracts with your medication. It is desirable to have a bath before surgery.